;)
Mobile Medical Clinic | Dump Light

After working with Aaron Brown and Caroline McDonald on the beginning stages of our mobile medical unit, I broke off and started a new analysis of program and needs of a Haitian mobile medical clinic moving around Haiti.
I found that we had already addressed several important issues; however, I decided to make a few changes.
INSERT PIC OF WALL
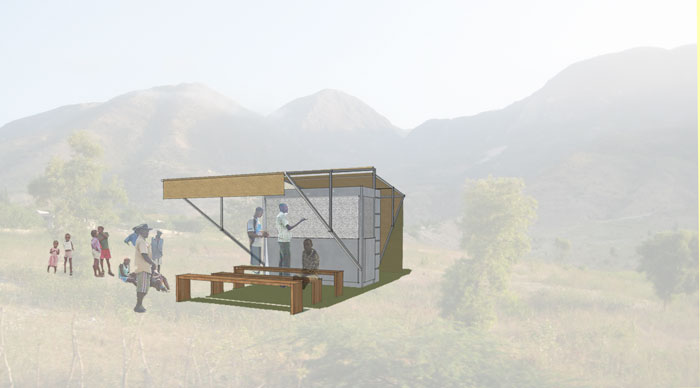
I created a smaller version of our original ‘Dump Truck’ design, one that could be more applicable and in use in a more common way. The size made it more accommodating for any regular size bed of a pick up truck. It was meant to be (mostly) of a steel material, and once planted onto a site, it was designed to unfold into a multi space unit.
;)
Because Haiti’s medical experience is several years behind the United States and our techniques and processes, I had to take numerous things into consideration. There, the pharmacy is meant to be separate from the actual medical examination process. I took this into account by allowing the actual original unit to become the secured pharmacy one arrival, helping to separate the check in/waiting area from the examination area.
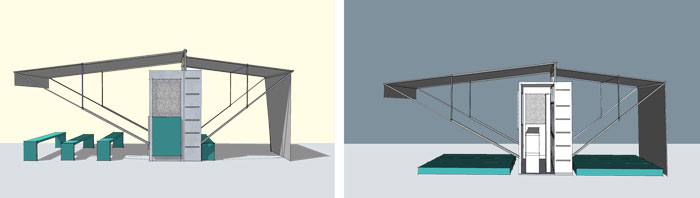
Since this specific design is reliant on a vehicle, I provided an option for non-truck use, which would include using the main shelf wall located within the actual unit. The wall would actually be composed of backpacks with drawers and shelves, meant to remain on the wall, but with the possibility of pulling out and being carried on individual’s backs.
;)
One of the main critiques I have come across with existing mobile clinics around Haiti is that most of them are designed to last a day, and there are well over double the amount of people that actually need to be seen. With this, the overall unit is meant to act as a multiday clinic, stocked with supplies to last for 4-5 days. Personal supplies for the workers and people visiting the clinic will be stored inside the unit and pulled out and used when needed (cots, benches, chairs, work surfaces).
 Lauren Metts
Lauren Metts